See original post here.
A typical pregnancy lasts about 40 weeks. Roe v. Wade, the Supreme Court decision that created a constitutional right to abortion, was reversed less than six months ago. This means the U.S. is currently at a unique inflection point in the history of reproductive rights: early enough to see the immediate effects of Dobbs v. Jackson Women’s Health Organization—closed clinics, a rapidly shifting map of abortion access—but too soon to measure the rise in babies born to mothers who did not wish to have them. Many of these babies will be born in states that already have the worst maternal- and child-health outcomes in the nation. Although the existence of these children is the goal of the anti-abortion movement, America is unprepared to adequately care for them and the people who give birth to them.
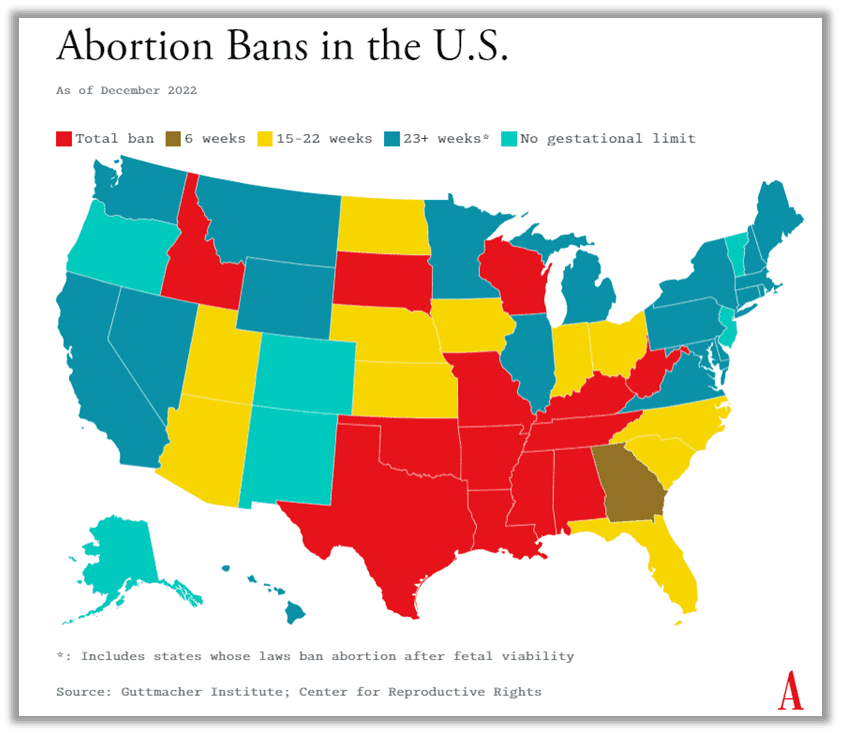
Much depends on how many states institute abortion bans and whether the bans are upheld in court, Caitlin Knowles Myers, an economics professor at Middlebury College, told me. (As of this writing, 13 states have near-total abortion bans, and more than 65 clinics have stopped providing abortions. A recent report by the Society of Family Planning found that legal abortions decreased 6 percent nationwide in the two months following the Dobbs decision.) But if the 24 states predicted to outlaw or severely restrict abortion do so, Myers estimates, there will be approximately 50,000 additional births nationwide.
According to her projections, about 42 percent of U.S. women of reproductive age will experience a change in distance to the closest abortion clinic. About three-quarters of people forced to travel farther to an abortion provider will find a way to do so, despite the distance. But a quarter will not. Of those, some will self-induce an abortion, some will miscarry, and some will go on to give birth.
When you consider that there were more than 3.6 million births in the U.S. in 2021, an increase of 50,000 births, or 1.4 percent, may not seem that significant. But these births won’t be equally distributed among the population; they’re likely to be concentrated among the poorest of the poor, in states where the social safety net is frayed to begin with.
“This is really an inequality story about who ends up trapped by distance and poverty, and who doesn’t,” Myers told me.
Many Republican governors in states where abortion has been banned have acknowledged that a baby boom is on the horizon, and that people obstructed from obtaining a wanted abortion will need additional help. “We absolutely must come together like never before to support women and teens facing unexpected or unwanted pregnancies,” Governor Brad Little of Idaho said in a statement. Some have framed the need to improve services for pregnant women and children as an important part of an anti-abortion agenda. But as of now, the actual plans in place to do so are staggeringly thin.
In Ohio, where a six-week abortion ban is stalled pending a court battle, Governor Mike DeWine has proposed eliminating the tax on diapers and baby supplies, and expanding Medicaid eligibility for pregnant women and children by raising the income limit to up to 300 percent of the federal poverty level. In Mississippi, Governor Tate Reeves has implemented a new tax credit for contributions to crisis pregnancy centers. In Texas, the health department has launched a new website to connect expecting parents to local resources. But these piecemeal solutions are insufficient; they fail to grapple with the severity of the situation for pregnant people and their children.
It’s not hard to prophesize the outcomes for those too constrained by their circumstances to leave their home state for an abortion. Previous research has shown that women who want to terminate a pregnancy but are turned away end up worse off financially than women who receive a wanted abortion. They are more likely to rely on public assistance, struggle to pay for basic living expenses, take on debt, and face eviction. This instability isn’t fleeting. For four years after being turned away, they will remain, on average, poorer than those who were able to obtain an abortion.
Money, of course, is only part of the equation. Pregnancy puts tremendous physical stress on a person’s body: People are estimated to be 14 times more likely to die during or after giving birth than from complications from an abortion.
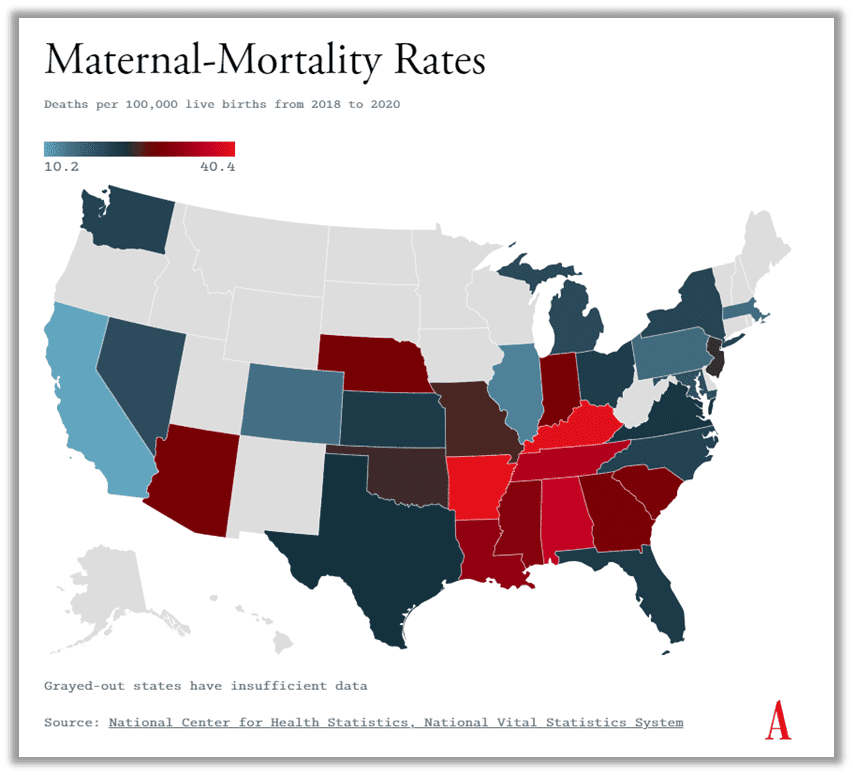
And the U.S already has striking racial disparities in maternal-mortality rates, with Black women nearly three times more likely to die from pregnancy-related causes than their white counterparts, according to the CDC.
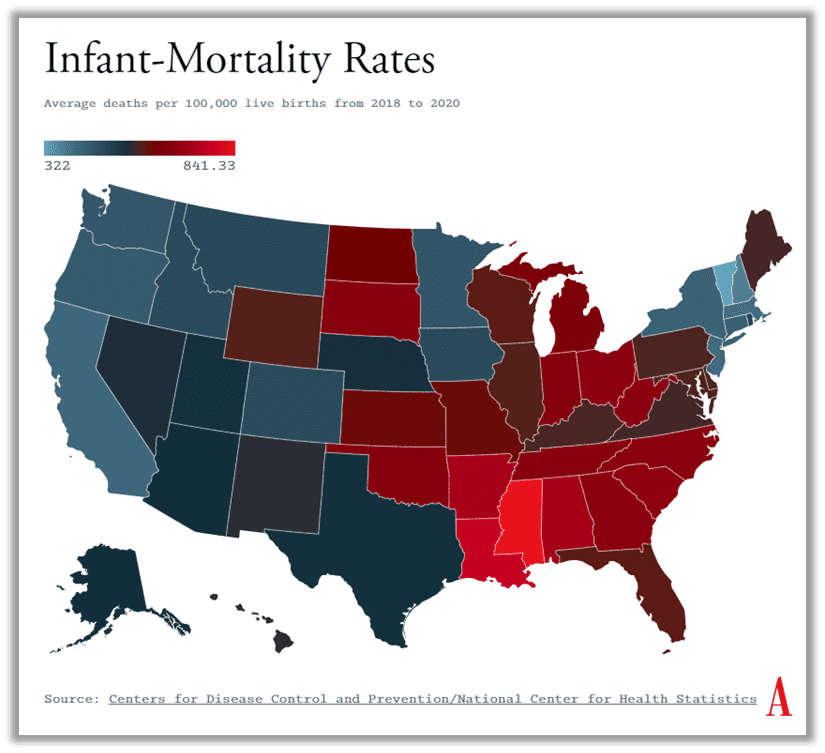
A similar disparity is seen in infant-mortality rates. And, compounding matters, many of the states that have banned abortion—such as Alabama, Arkansas, Kentucky, Louisiana, Mississippi, Missouri, Oklahoma, Tennessee, and Texas—also happen to be among the states where mothers and newborns fare the worst. If you look at the six states with the highest maternal-mortality rates in the nation according to the CDC, for example, all of them have outlawed abortion in the past few months. The same goes for the six states with the highest infant-mortality rates.
A prime example is Arkansas, which is ranked the “most pro-life state in the U.S.” by Americans United for Life, a group that opposes abortion. Minutes after Roe was overturned, Arkansas outlawed abortion in all circumstances except to save the life of the pregnant woman. As a result, the state is expected to see a 3 percent increase in births, or an average of 1,000 extra births a year, according to Myers’s research.
Arkansas already has the highest maternal-mortality rate in the U.S., nearly double the national average. If no one in Arkansas were able to receive abortions, the maternal-mortality rate would be expected to spike an additional 7 percent, according to research from the University of Colorado at Boulder. “We already have a limited number of ob-gyns,” says Lori Williams, the board chair of the National Abortion Federation and the former clinical director at Little Rock Family Planning Services, an abortion clinic that has since closed. “We already have a limited number of places for these patients to deliver and physicians to care for them. And now we’ve intensified the problem without a preplanned solution.” Arkansas is not an outlier here: According to a new report from the March of Dimes, about 35 percent of U.S. counties, mostly clustered in the Midwest and the South, are “maternity care deserts,” which means they do not have a hospital that provides obstetric care, a birth center, or any obstetric providers.
Asa Hutchinson, Arkansas’s Republican governor, has acknowledged the challenge ahead. “A state that aspires to be pro-life must protect the most vulnerable at every stage of life,” he said in an address in August. He has pledged to expand some of the services that pregnant women and new mothers can receive through Medicaid and to increase payments to foster parents, and he announced a new phone line, 1-855-ARK-MOMS, to direct pregnant people to resources in their area. But a hotline connecting pregnant people to resources is only valuable if the resources are available—and if prohibitive policies don’t stand in the way of parents qualifying to receive them in the first place. And Arkansas’s track record on social services is not encouraging.
Arkansas has the second-highest food-insecurity rate in the country—but as Laura Kellams, the Northwest Arkansas director of Arkansas Advocates for Children and Families, explained to me, restrictive Supplemental Nutrition Assistance Program policies make qualifying for food stamps hard for those in need.
A dismal four out of every 100 families in poverty have access to the state’s cash-assistance program, Temporary Assistance for Needy Families.
According to a recent ProPublica investigation into how states spend federal welfare funds, Arkansas—along with Texas, Mississippi, and Nebraska—denied about 90 percent of applicants in 2020. Arkansas is ranked among the worst states for child well-being, according to an analysis from the 2022 “Kids Count Data Book.
”It has the highest rate of teen births in the country, according to the CDC, roughly tied with Mississippi, and does not require sex education to be taught in schools.
One thing states can do if they want to address high maternal-mortality rates is extend Medicaid coverage for women to a full year after they give birth. Currently, federal law requires states to provide pregnancy-related Medicaid coverage for two months postpartum. However, states have the option to apply to extend coverage to 12 months, through a provision in the American Rescue Plan Act of 2021. Some states that have banned abortion, such as Alabama and Kentucky, have taken steps to expand coverage in the name of improving women’s health. But 14 states that are expected to or have already banned abortion have not. Earlier this year, Republican legislators in Mississippi, which ranks sixth-worst in the nation in maternal mortality and the worst in infant mortality, defeated an attempt to expand coverage for postpartum women. (Mississippi state health officials have predicted an extra 5,000 births a year due to the overturning of Roe.)
Andrea Miller, the president of the National Institute for Reproductive Health, told me that she is not optimistic that states historically opposed to abortion will now embrace policies benefiting pregnant women and children. “They have had decades and decades to do things about that, and have taken few, if any, steps,” she said, adding that any increase in births will inevitably put pressure on overtaxed health-care and social-service systems. “We are not seeing anything that dramatically changes that.”
Anti-abortion politicians have said that the next phase of the movement is to support pregnant women and families, which raises the question: What would it mean to truly do so? If we dare to dream big, a map for the country’s post-Roe future could include investment in not only comprehensive health-care and mental-health services for pregnant and postpartum people, but also a living wage, paid family leave, subsidized child care, and affordable housing. On the preventive side, we could focus on comprehensive sex education in schools and access to contraceptives.
But months after the end of Roe, there’s little evidence that many politicians have a genuine interest in the types of policies that would make a pronounced difference in the lives of pregnant women and children.
Websites and hotlines are no match for the problems the U.S. now faces. We know what’s coming: More babies will be born into poverty. Some women will die. More will be thrust deeper into financial insecurity. The social safety nets that do exist will likely be pushed to their breaking point. If we accept that there will be about 50,000 more births, that means we have 50,000 more chances to invest in pregnant women and support their newborns. Unless states that have banned abortion proactively strengthen the social safety net, the future prospects of these post-Roe children and their moms are unsteady at best. If this moment is a test for the anti-abortion movement, then it has not yet passed.